“Don’t React – Choose How to Relate to Distressing Voices!” is the subject of a webinar that was presented by Dr. Mark Hayward on 6/20/19. (See the link to the complete recording below.)
This webinar presents a very practical way to help people start experimenting with different ways of relating to voices they might be having trouble with. I encourage people to check it out!
“There has recently been a shift from conceptualizing a voice as a sensory stimulus that the hearer holds beliefs about, to a voice as a person-like stimulus which the hearer has a relationship with. Understanding voice hearing experiences within relational frameworks has resulted in the development of psychological therapies that focus upon the experience of relating to and with distressing voices. This webinar explores lessons learnt from the development, experience and evaluation of one of these therapies – Relating Therapy. These lessons are located within the broader context of other relationally-based therapies that seek to support recovery through the use of digital enhancement (Avatar Therapy) and dynamic interaction with voices (Talking With Voices).”
About the presenter: Mark Hayward has worked
as a Clinical Psychologist within NHS mental health services for the past 20
years. His roles combine clinical (Lead for the Sussex Voices
Clinic), research (Director of Research for Sussex Partnership NHS
Foundation Trust) and teaching (Honorary Senior Research Fellow at the
University of Sussex).
His
research activities have focused primarily on the exploration of voice hearing
within relational frameworks – acknowledging the voice as an interpersonal
‘other’ and researching differing aspects of the relationships that people can
develop with their voices. These relationships have been central to the
development and evaluation of new forms of individual and group therapy that
can facilitate acceptance of self and voices through the use of assertiveness
and mindfulness training. His books include the CBT self-help book ‘Overcoming
Distressing Voices’, and the research monograph ‘Psychological Approaches to
Understanding and Treating Auditory Hallucinations’.
Mark
is committed to increasing access to effective psychological therapies for
people distressed by hearing voices.
I’ve been intrigued by the way the battle against mental health system oppression has drawn on two important and powerful ideas – which happen to contradict each other!
One is the idea that people can “recover” from mental health problems. Asserting the possibility of recovery has been key to fighting back against the oppressive belief that certain people will always be “mentally ill” and will need to resign themselves to a limited life as a mental patient, etc.
The second idea is that people may not have to change to be OK and valuable – that people can even be proud of what has been called madness! Mad pride helps people fight back against the oppressive notion that one has to be “normal” to be acceptable, and that mental diversity means illness.
But, if one is perfectly OK as one is, then there is no need for recovery. In fact, if one is already quite OK, then the suggestion that one should work on recovery can itself be oppressive – like offering “reparative therapy” for gay people.
On the other hand, if one’s mental state and current beliefs are causing lots of problems that are keeping one stuck, then being encouraged to be proud of that mental state can become a barrier to changing or recovering and so can deepen or prolong problems and oppression.
Contradictions like those outlined above can lead to battles between activists about how to move forward. They can also lead to battles, and confusion, within people who are trying to find the best way to deal with their own “mad” states.
What I want to show is that it’s possible to embrace both “recovery” and “mad pride” despite the contradictions. But to do so, we need to be aware of both the advantages, and of the “down” or “shadow” side of each of these notions.
Compared to mad pride, recovery has been much more widely embraced. It has even been embraced by much or most of the mental health system – though often what is embraced is just the word itself, and not the possible reality! But because of its popularity, it has also been more widely critiqued, and some have even advocated that we stop using the word altogether.
One common critique is that the word “recovery” implies that one must have been ill in the first place, and so this word should not be used when the problem never was an “illness.” However, people do “recover” from many things that aren’t an illness: we recover our balance, we recover from injuries, we even recover from the down side of events that were overall positive, as in “I’ve finally recovered from that wild party I attended last night!” Krista Mackinnon, in her “Recovering Our Families” course, emphasizes that all humans are constantly recovering from all sorts of things, and so “recovery” is not something unique to those who have been psychiatrically labeled.
A stronger critique of the notion of recovery points out that recovery involves going back to something, while many prefer to see their life as going forward. John Herold for example talks about wanting to move toward “discovery” and not “recovery.” I agree with that up to a point, but I also notice that we often have to go back to something we had possessed previously in order to move forward overall. For example, if I used to know how to face people and maintain friendships, but then I seemed to have lost that ability during an emotional crisis, I may want to recover the skills and habits I had before so that I can then get on with my life and move into that wider process of discovery.
Then there’s the problem of the word being co-opted to mean something much less than real recovery. Lots of mental health programs use the recovery word, but their practices remain targeted towards lifelong drugging and containment of the person, with “recovery” apparently meaning only getting to where the person won’t be in crisis so much. I understand why that sort of use of the word “recovery” makes people want to vomit, but I would rather work on reclaiming the word, rather than giving it up. The US government can call a nuclear missile a “Peacekeeper” but that doesn’t mean we need to quit using the word “peace.” I think our best strategy is to continue to emphasize the true meaning of recovery and to contrast truly recovery-oriented treatment with that which is not.
Adding complexity to discussions of recovery is the distinction between “clinical recovery,” or no longer experiencing “symptoms,” versus “personal recovery” which has been defined as “recovering a life worth living.”
Interestingly, within standard care, “personal recovery” is often framed as the proper goal because of a belief that “clinical recovery” is not possible. In other words, it is believed that the person will always have symptoms and will always be less than healthy than others because of that, but they may still learn to “recover a life worth living” despite continuing to be ill. (Of course, this notion that they are still ill can be used to convince people to stay on their drugs, which makes this interpretation popular amongst those who embrace the medical model but who still want to offer some appearance of hope.)
But there is a deeper and more valid reason to focus on personal recovery rather than clinical. That’s because the experiences that the mental health system called “symptoms” may not be a problem at all once the person learns to live with them. Hearing voices for example may be benign or even helpful once the person learns to relate to them differently. And once experiences no longer cause problems, there is no longer a need for drugs or any kind of treatment to manage them.
Of course, it’s the idea that people don’t need to change, and that their differences may be OK or even something quite valuable, that is basic to that idea that sometimes seems in opposition to recovery: mad pride.
“You are only given a little spark of madness. You mustn’t lose it.” Robin Williams
From a radical mad pride perspective, there is only mental diversity, and not any mental problems, disorders, or illnesses. People do best when they accept and become proud of themselves as they are rather than try to change. If people have problems, or seem to be disabled in some way, it’s just because society has failed to accommodate their differences, and so it’s society that needs to change.
But what are the problems with this kind of radical mad pride perspective?
One issue is that if I am suffering in some way, while believing that there is nothing wrong with me but only problems with others, and if it’s also true that I don’t have the power to make others change, then I am stuck with my suffering. Working on recovery from a problem may not require accepting that one is ill, but it at least requires accepting that something needs to be changed; but pride is the opposite of believing in a need for change.
Another problem is the adversarial relationships that a radical mad pride perspective can create with others. If I for example demand that others change their attitudes and start accepting me just as I am and if I demand that they change in other ways to accommodate my differentness, while I insist that I am perfectly fine as I am and don’t need to change anything, I may just piss people off. I’m certainly not likely to be effective at winning friends and forming peaceful relationships, since good relationships tend to be built when people are willing to change at least some to accommodate each other, at least when they are able to do so.
On the other hand, the notion of radically accepting ourselves just as we are can often seem to be the very core of peace of mind and mental healing. So it can all seem quite complex.
How can all this be best resolved? Or, how can we take what is best about mad pride, and what is best about recovery, without getting caught up in the shadow side of each?
I think it may help to take a step back, and look in more general terms at how we can resolve other kinds of contradictions.
It’s not uncommon that things are opposites, but we find ourselves needing both. Breathing in for example is a good thing, but so is breathing out, even though that’s the opposite. Our ability to open up to people and trust is a good thing, but so at certain times is our ability to close up and distrust.
Mental health issues can be notoriously complex. People can go through terrifying, bewildering experiences that may also have a very important positive side. Or, experiences may seem to be quite positive, but then lead to something very detrimental.
It’s also possible that an experience we want to recover from at one point may be something that later we wish to regain. In my own life I can identify times I have worked to recover from “madness” and to regain my ability to integrate with normality, and then also times when it seemed more important to turn around and work to recover from that normality trance, so I could reclaim what I had discovered when I first went “out of my mind.”
One metaphor for madness is that of revolution. Revolution overthrows the existing order – then anything is possible, which is both great, and terrible. Revolution is both something to be proud of, when it is necessary and when it works out well, and it is something to recover from, so that order can be restored.
When we over-value sanity, we stick with an existing order in rigid ways that can be oppressive. When we over-value madness, or revolts against sanity, we can get lost in disorder. Life though works best at the edge of chaos and order, so it may require both rebellion against order and efforts to recover order.
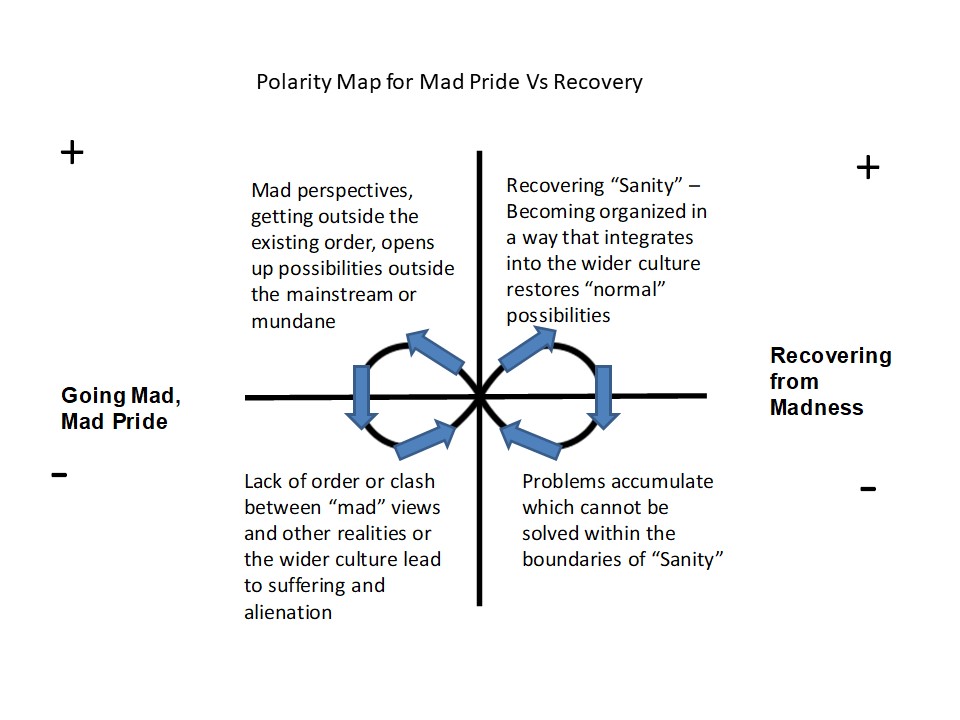
One way to map relations between polarities, where neither polar opposite provides a full answer, is to use what is called a polarity management map. These maps make overt what is positive and negative about each polarity, and suggest that each polarity is the solution for the problems caused by the other.
Below is a polarity management map about recovery versus mad pride. It suggests that there is no final answer to resolving the tensions between mad pride and recovery, or between madness and sanity generally. Rather, whenever we emphasize the positive of one side, we will also sooner or later encounter its negative, and then may have to shift to the opposite side.
If we follow this line of thinking, it follows that there are no final answers as to when a focus on change and recovery is best, versus when it might be better to instead be proud of one’s current state and perspective, even if it is somewhat “mad.” Instead, we will be more open to exploring what might fit or seem healthy, or not, in any given situation. And we will be open to the possibility that whatever we choose now, we will later be called upon to choose the opposite.
When we are too sure that our side is right, that “God is on our side,” we end up at war with our opposite. People who are too sure that their current mental view or version of sanity is correct will go to war against that which opposes it, be they voices or other people who are seen mentally wrong But going to war just makes everything more extreme, and prevents the “peaceful revolutions” that are possible when people realize that their current polarity is just one side of a more complex picture.
Modern humans are not, of course, the first to struggle with these issues. Spiritual traditions going back to ancient times wrestle with how to relate to the limits of any existing order, and how to find value in what is outside of that order, or “outside of our minds.” While these traditions are not perfect, and have too many times been bent to completely corrupt and oppressive purposes, they also contain reminders that we humans do our best not when we stay confined within a mundane “sanity” but rather when we allow ourselves, at least at times, to open up to what goes beyond.
What would mental health treatment look like if it balanced an awareness of the need for “recovery” with an awareness that people also sometimes need to go “out of their minds” to resolve problems that they haven’t been able to solve otherwise, or maybe that their entire culture has not been able to face and resolve?
To explore some possible answers to that question, I recently put together a new online course, “Addressing Spiritual Issues Within Treatment for Psychosis and Bipolar.” This course outlines some radically different ways of conceptualizing the mental states that get called “psychosis” and “bipolar” and reviews ways professionals can shift from pretending to “know it all” to being helpful to people as they face some of the bigger mysteries together. In the course, I try to strike a balanced position that avoids both “romanticizing” extreme states and the more common mistake of “awfulizing” or “pathologizing” them.
This course comes with 6 CE for most US professionals. Use this link to get more information, or to register.
A few more thoughts:
One other possibly helpful metaphor for madness is that of wilderness.
It can be disturbing when young people wander off into the wilderness. What if they become lost, and need to be rescued? Sometimes people do need to be rescued. But a society too sure that the wilderness is nothing but bad will seek to prevent young people from ever wandering off, won’t recognize when people are doing OK in their explorations and don’t need to be rescued, and/or will even seek to destroy the wilderness so that everything can be “civilized” – aka, sane.
But any society cuts itself off from the wilderness, and/or declares war on what is wild, only at its own peril. Certainly, modern civilization or “normality” has declared war on the wild, and it does often seem that it is winning. But that “winning” is a most terrible thing, and puts us all in danger!
Rather than winning, we need to focus more on finding a dynamic balance, or peaceful coexistence. The peaceful coexistence between recovery and mad pride that I have proposed is just one example of that.
Emerson said that “People wish to be settled; only as far as they are unsettled is there any hope for them.” It’s time that we define mental health not as some settled “sanity” but as the unsettled and possibly playful dialogue that results when we value both madness and sanity, and when we explore together with those whom we wish to help rather than impose our own version of some settled, and dead, “correct answer.”
When people have problems with voices, the most common recommendation they are given is to try to avoid them – to take drugs to make them stop, to simply ignore them, to use distraction, or similar approaches.
But these strategies often don’t work. Or even if they do seem to work, they may themselves cause other kinds of problems that may not be acceptable. So what else can people try?
One possibility is to try the opposite of avoidance: to deliberately engage with the voices!
But this sounds scary or wrong to some people. Won’t engaging with the voices make people take them too seriously or see them as more real than they are? Might that lead to people getting even more lost in the world of voices, and so more distressed?
While the mind is tricky and things can always go wrong, we now know that it is possible for people to engage with voices in ways that make things better. Specifically, when the engagement is done with creativity and compassion, the result can be a positive change in the relationship with voices, leading to much greater peace of mind.
But how can people learn how to facilitate this sort of constructive engagement?
Fortunately, Charlie Heriot-Maitland (known for producing the Compassion for Voices video), Rufus May, and Elisabeth Svanholmer have just made available a free series of videos, in which they offer practical ideas about how to do just that. These videos cover topics such as how to:
Prepare to engage with voices
Identify and nurture the compassionate self and engage with voices from that perspective
Change the power balance with voices
Identify the function of voices
Work with voices that don’t seem to want to engage
Map out voices
Engage constructively with voices that sound like an abusive person from the past
Marital arts exercises that can help in work with voices
I spoke to Rufus May, one of those involved in making these videos, and asked him what inspired he and his colleagues to do this. He answered that:
“We know there is a growing interest in this approach and we wanted to make some accessible resources. In the Bradford Hearing Voices group I volunteer with, I might facilitate a dialogue with a group member’s voice and then encourage them to regularly engage with their voice or voices. In this way group members have found they have been able to improve the relationship they have with their voices.
“People ask me, how can you talk with someone’s voice? I sometimes joke ‘I‘ve got a special microphone!’ But the truth is we ask someone to ask their voice questions and then report the answers the voice is giving them. We have found if we use good communication skills such as empathy and non-judgemental questions the voice sometimes begins to respond in a different way.”
I asked Rufus for an example of this:
“Through a facilitated dialogue with a person’s voice that was being quite harsh and critical towards the person, we established the voice wanted the person to be more assertive with people in their social network. The person went on to consult with the voice on who to be more assertive with and when she became more assertive the voice seemed to relax and become more constructive.
“We have also found if people compromise with their voices the voices often behave in a less controlling way. So finding out if the voices like certain types of music or food or drink and listening to the music the voice likes or consuming the food the voice likes can role model to the voices a more respectful collaborative relationship.”
I asked Rufus where these engaging approaches have come from:
“In many traditional cultures consulting with voices is something that has been done for 100s of years. The original Hearing Voices research carried out by Romme and Escher in the 80s in Holland found many voice hearers who had never used mental health services negotiated and engaged with their voices.
“The challenge is how to talk with voices that are hostile and controlling. This means we as communities need to support voice hearers to become more confident in being assertive with their voices and then learning how to engage in a power with style of relationship, rather than power over.
“Hearing Voices groups can be good spaces to learn this ‘living with voices’ approach. We have also found tools like Nonviolent communication and mindfulness and compassionate mind exercises helpful in supporting this process.
We have tried to make short films that demonstrate how you can engage voices and find ways to learn from them. The three of us myself, Elisabeth and Charlie have used both role-play and some demonstrations of mapping out and talking with Elisabeth’s voices.
“We don’t want engaging with voices to become a therapy that only highly trained professionals can used. While we welcome therapists using these approaches, we also want people who hear voices, and their friends and family to know about dialoguing and creative ways to understand and engage with voices.”
I think that last point Rufus makes is really important! It’s helpful when mental health professionals can offer certain kinds of assistance, but it can be even better when people learn how to help themselves and each other. That’s what really creates a healthy society. So I hope lots of you take an interest in this approach and do check out the video series, which again is available at https://openmindedonline.com/portfolio/engaging-with-voices-videos/
” The approach is not so much trans-diagnostic as dismantling of diagnosis, and includes a perspective on psychosis that sees it as part of a wider potential of human experiencing that includes valued aspects such as spirituality and creativity.”
What would it look like if mental health providers were
trained to be both deeply humanistic, AND very efficient at helping people
identify and cope with the issues at the core of whatever their difficulties
might be, including psychosis?
It might look like the approach developed by Isabel Clarke and Hazel Nicholls, which they call “Comprehend, Cope and Connect (CCC).” CCC starts from the perspective of the immediate experience of the individual -‘what it feels like to be me, now’. This approach to mental health difficulties brings together the impact of past trauma and adversity on present coping (comprehend), and utilizes the latest in mindfulness and compassion-focused approaches to manage change (cope and connect).
In the presentation linked to below, Isabel Clarke focuses on using this approach with people whose experiences might be described as “psychosis.” Isabel brings a uniquely deep and yet practical understanding to this topic. On the one hand, she has thought deeply about the nature of psychosis, and she has written several inspiring and insightful books and articles on the intersection of spirituality and psychosis. On the other hand, she has extensive experience working in acute care settings where making a direct an immediate impact is essential, and this has pushed her to develop an approach capable of accomplishing that objective.
“Simple and yet powerful, this impressive body of work has
transformed practice wherever it has been introduced. Mental health practitioners
should all be aware of it.” said Dr Lucy Johnstone, consultant clinical
psychologist and author of ‘Formulation in psychology and psychotherapy’.
Comprehend, Cope, Connect: An Experience Based Approach to Psychosis & Other Mental Health Challenges
About the presenter:
Isabel Clarke’s work spans two areas: psychosis and
spirituality, and clinical psychology. Both draw on the research based Interacting
Cognitive Subsystems model of cognition, and both seek to bring spirituality
into center stage, founding it in cognitive and other research and theory, and
regarding it as a central part of what it means to be human.
Recently Isabel has been developing Comprehend, Cope and
Connect (CCC – previously known as Emotion Focused Formulation Approach,
EFFA) in the diverse contexts of Acute, Primary Care and Culture Free
Adaptation. See “ICS Underpinning 3rd Wave CBT” and
the following book for more details:
Clarke, I. & Nicholls, H. (2018) Third Wave CBT
Integration for Individuals and Teams: Comprehend, Cope and Connect.
London & NY: Routledge.
Other books by Isabel Clarke:
Clarke, I. (2013) Spirituality: a new way into understanding
psychosis. In E.M.J. Morris, L.C.Johns & J.E.Oliver Eds. Acceptance and
Commitment Therapy and Mindfulness for Psychosis. Chichester:
Wiley-Blackwell.P.160-171.
Clarke, I. ( 2008) Madness, Mystery and the Survival of God.
Winchester:’O’Books.
Clarke, I. (Ed.) (2010) Psychosis and
Spirituality: consolidating the new paradigm. Chichester: Wiley
When someone is “mad” or “psychotic,” should the people around them try to make sense of their experience and of what they are saying? Or should the person be taken to professionals who will listen only in order to diagnose and then prescribe treatments aimed at suppressing or eliminating experiences that are understood to be meaningless?
In the mainstream of mental health treatment in the US, the latter approach is dominant. But what does it mean to be “treated” by people who won’t try to understand you?
When I was a young man having experiences that were “extreme” and arguably quite “mad” or “psychotic,” one of my worst fears was that the people around me would give up on the idea of finding any significance in what I was communicating, and that they would decide to see it as something that simply couldn’t, or even shouldn’t, be understood.
Fortunately I always seemed to keep some contact with at least one person who saw some significance or meaning in what I had to share, and after awhile, I made more sense of it myself and had a better time communicating with others. Now I work as a therapist, helping others explore the significance of their own “mad” experiences.
I was recently interviewed on the topic of “Finding Meaning in Psychosis.” You can check out that interview here:
Thanks to Stacy Duffy for being the interviewer! Also thanks to everyone at Psychosis Summit who contributed to making this happen. (There are 20 additional interviews with a wide variety of perspectives and innovative approaches to psychosis at the Psychosis Summit website, https://www.psychosissummit.com/ )
Cognitive therapy is probably still understood by most to be about trying to reduce or dispute “thinking errors” or such. But last week, at the ISPS-US conference, I had a chance to hear from Aaron Beck and his team (Beck is still quite active at 97 years old!) and it was interesting to see just how much they have moved toward evoking something positive as their first priority.
Aaron Beck at 97 years old, presenting at the 2018 ISPS-US conference, alongside his colleague Ellen Inverso
Beck’s current work is recovery oriented cognitive therapy for psychosis. They see the core of the work as being finding ways for people to have experiences that give them or help them find a sense of meaning, connection, and purpose. Their overall aim is still to change beliefs, especially the “self defeating beliefs” that lead to “negative symptoms” but they see those beliefs as often falling away as people have access to the positive stuff.
Beck overtly stated that therapy should be person centered, not symptom centered (even though so much CBT is the latter.)
I really liked lots of the examples given about how to be person centered even when faced with challenging stuff. For example, one person in the audience asked how to talk with a guy who claimed to have been roasted in an oven. Beck said first he would acknowledge the story, then he would be curious about what that was like, how he felt etc., then he would ask about other times in the person’s life when he may have felt that way, or does anything currently make him feel that way. It seemed he was describing a process of following the vein of emotional content to where it would connect with more realistic biographical facts or current issues.
Beck stated that helping the person get going with something positive, something that has meaning and purpose for the person and gives them a sense of connection, tends to “suck the juice out of” any delusion.
He was also very much into discovering the wants and needs behind even very challenging behaviors. One story was about a doctor trained in recovery oriented cognitive therapy, who had a patient who was saying he wanted to shoot him. So instead of treating it as a symptom, he asked the patient, “why do you want to shoot me?” The patient responded, “because you are planning to shoot me.” “But,” the doctor explained, “I don’t even own a gun!” “Well,” said the patient, “you use your drugs like a gun.” The doctor thought about it and said, “I wonder if you are feeling you have very little control? That must be frustrating. But I know you must have lots you want to do outside of here and I want to help you get out so you can do that!” This made sense to the person and they started to work together.
One good introduction to recovery oriented cognitive therapy for psychosis is the following recorded webinar:
In addition, SAMSHA now has available a series of webinars that goes into more detail about this approach, at this link.
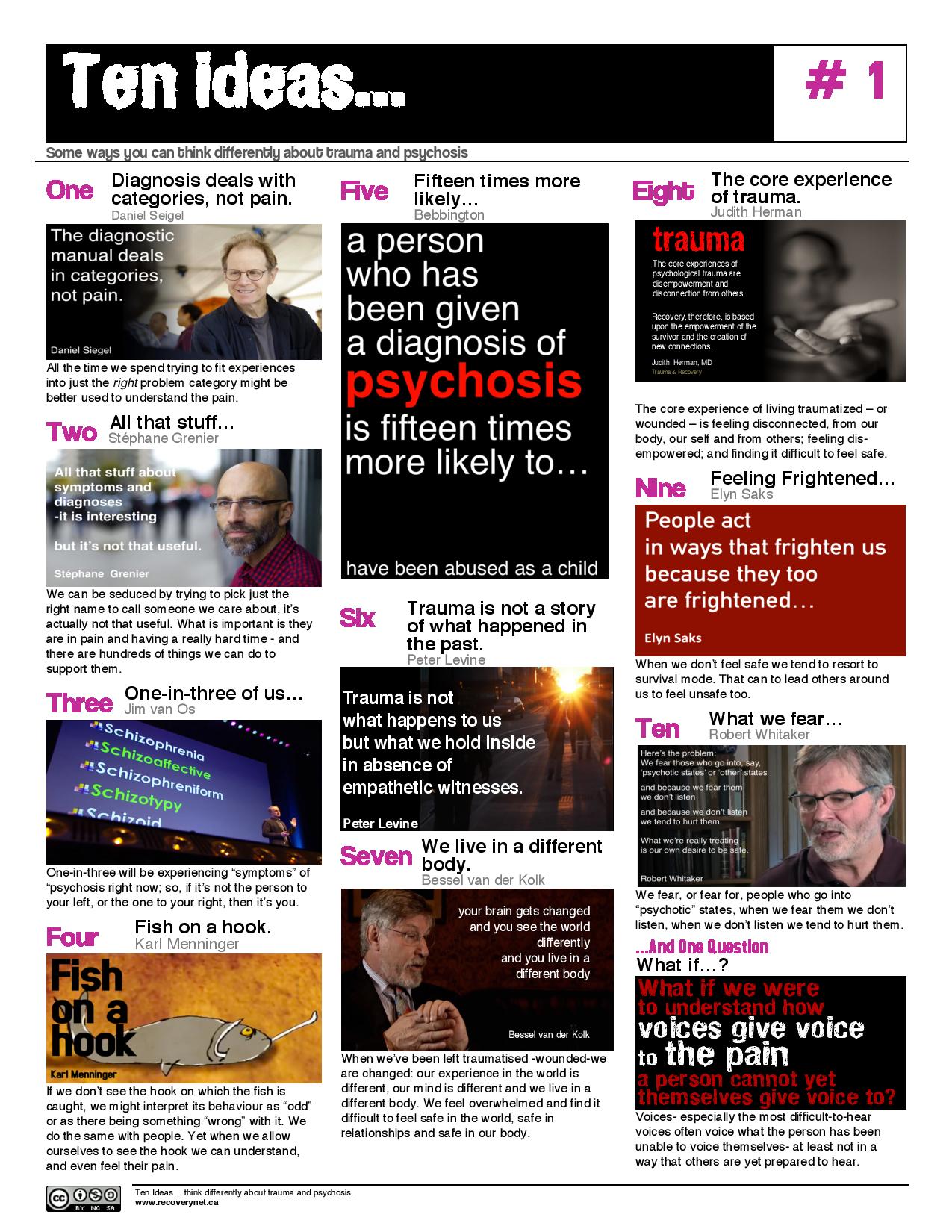
A colleague recently suggested to me that one of the very worst (yet common) practices in modern mental health treatment is the one of telling people that their psychotic confusion is just something wrong with their brain, and that it should not be understood as a response to something that happened to them.
When that happens, an already confused person can easily become more confused as the link between traumatic experience they might have had, and their confused response to that experience, is denied and becomes invisible.
One way to challenge that thinking is just to download and print this flyer, which describes ten ideas for thinking differently about trauma and psychosis. Lots of great food for thought all on one page! Thanks to Recovery Network: Toronto for putting this together.
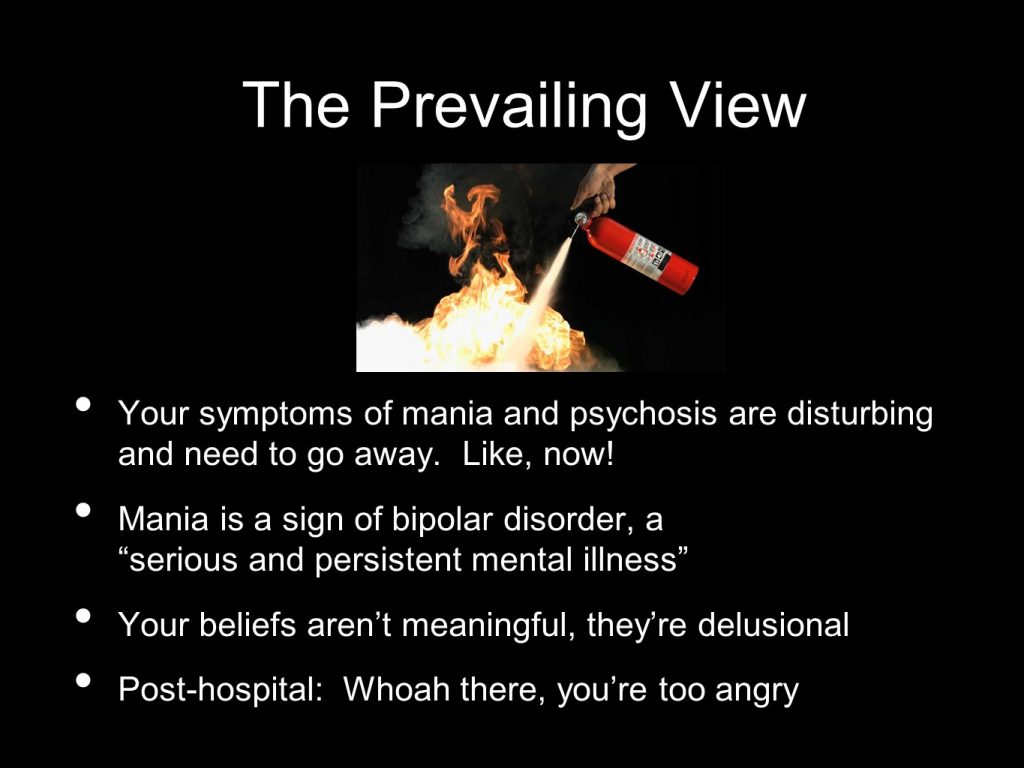
My colleague John Herold has an interesting image he uses to communicate the conventional mental health approach to disturbing mental states: it is that of a fire extinguisher being applied to a fire.
If we think of disturbing states as an illness, then it makes sense that we focus on trying to eliminate them or to “put them out.” Of what use is an illness?
But what if these states are something more than that? A key alternative idea is that disturbing states represent something important that is trying to emerge, something that has been missing from our dominant mental states. We may not know yet how to integrate it, but the possibility of getting to know it better, of making peace with it, and finding value in it, exists.
I believe it makes more sense to conceptualize “psychosis” as something like a revolution in the mind, than as an illness. And as John F. Kennedy famously said, “Those who make peaceful revolution impossible will make violent revolution inevitable.” It follows then that if we want to make “psychosis” less disturbing, we need to focus less on suppression, and more on actually facilitating altered states of consciousness and integrating them into our lives!
That’s the approach taken in Process Oriented Psychology, also known as Process Work.
When John Herold went to see a Process Work counselor, they talked about how John’s experience of extreme states had been too intense and had been disruptive in his life, and had led to hospitalization, something that John wanted to avoid in the future. But they also talked about how these states had value. The counselor then compared John’s experience with drinking an entire bottle of Tabasco sauce all at once. Why not instead, the counselor suggested, “try being just a little psychotic all the time?”
That strategy turned out to work great: applying it allowed John to make peace within his mind. In fact, it worked so well that John became inspired to get a diploma in Process Work and to begin teaching about it.
Conventional mental health approaches tend to be deadening — this isn’t surprising given that suppressing part of the psyche is their goal. Not so Process Work: it is always lively and playful, often playing specifically with that which has been disturbing. No mental state is taken as having the whole truth: instead, it is always possible to take any state to its “edge” and then over the edge, into something else. It’s an approach that very much values diverse mental states.
Another aspect of conventional mental health approaches is their tendency to assume that “reality” is a given, and that the goal should be to have everyone be in touch with it in the same way. “Consensus reality,” where everything can be divided up and measured, is the only kind of reality that is valued.
In contrast, Process Work sees reality as having a number of different dimensions, with some value in being in touch with different dimensions at different times.
“Dreamland” for example can be seen as a level of reality, or a way of being in touch with an aspect of reality. In process work, “dreaming” is not just something we do at night, but something that comes up in body sensations and symptoms, in fantasies, in visions and voices, etc. These experiences are “not real” from the perspective of consensus reality, but are completely real on their own terms.
Another level of reality is that of “essence”: this relates to the non-dual aspect of reality. At this level we can experience that we are all one consciousness, that there is no observer separate from the observed, and that all of reality can be experienced as right here right now.
This relates to my experience, as many of the most powerful events that shaped me did not take place in “consensus reality.”
One such event occurred when I was 17 years old, when I took LSD for the first time. I had the experience of going to another dimension, where I met some beings who told me I did not have to continue to be who I had been, that I could be a completely new person. This sounded great to me, because I did not like my self up to that point — it was too much shaped by fear, defined by people who had abused me. So I went with the new identity!
For the next 15 years or so, I continued to see my origin as more related to that “dreamland” event of becoming a new being, than it was to my “consensus reality” experience of growing up with abuse. I also focused very much on “essence level” reality, as that gave me a point of origin quite other from my childhood, and helped me continue to escape from feeling vulnerable.
This continued until various events, combined with my increasing awareness of the costs of denying my basic human vulnerability, pushed me to face my past and the dimensions of experience that I had disowned. This was at first shocking and very disruptive, and it seemed I was at risk of losing my sense of safety and being stuck in the trauma that I had previously avoided — at least until I got help in integrating from some competent therapists, one of whom had training in process work.
In Process Work, everyone is understood to have a “primary process” or a kind of functioning with which they identify, and also the possibility of having a “secondary process” which may disturb, or offer an alternative to, the primary process. When the contrast between the primary and secondary process is very sharp, there is the possibility of something they call a “process inversion” in which the two switch, and what was the person’s primary process now seems to be completely missing.
From this point of view, what happened to me when I was 17 was that I crossed over from what had been a primary process highly affected by trauma and abuse, to a secondary process of being someone who was fresh and unaffected by abuse. This was a “process inversion” because my past identity became missing, and I could not or would not relate to the person I had been. Turning to face my childhood trauma 15 years later threatened me with another such inversion, but after some rocky times I found ways to become more fluid and able to draw from both identities: the one who had been crushed by abuse, and the one who had never been touched by it.
An important aspect of Process Work is that nothing is pathologized; every part of the person, every kind of experience, is seen as having value. A process worker would see value both in my crossing over into being someone who never had a childhood, and also crossing back into reclaiming a very disturbing past. People may, as I did, get stuck in some parts of their experience and need help finding a way to be more fluid so they can also relate to other parts, but there is nothing that needs to be suppressed or gotten rid of.
Want to know more about the this approach? Then I suggest watching the video below, a very lively, recently recorded presentation by John Herold, who knows a lot more about Process Work than I do! In this presentation, he covers deep and complex topics with amazing clarity and humor, and he speaks informed not just by theory but with perspective drawn from learning to manage his own extreme states. After you watch it, please let us know what you think!
To find out more about John or to watch some of his other presentations, go to http://johnherold.net/
“Acceptance and Commitment Therapy” or “ACT” is a way of working with experience that focuses on just accepting difficult experiences while shifting attention to moving toward values. This approach can really help people improve the quality of their lives, often by making some fairly simple changes in their approach.
Eric Morris is a researcher and author who has developed some practical ways of teaching people this approach in a group format. So those of you who facilitate groups might be especially interested in hearing what he has to say in this webinar (recorded 5/31/18):
Stories organize us, and “bad stories” organize us in destructive ways. In this post I will address one example: the story told about how skilled mental health professionals can distinguish between dissociative disorders, with their roots in trauma, and psychotic disorders, which are understood to be definitely illnesses of the brain.
Why do professionals attempt to make such a distinction? The idea is that people with dissociative disorders need to be offered caring and skillful therapy which addresses their traumatic past and their fragmented response to it, so they can reorganize in a more integrated way. It is thought that such a psychological approach would be useless for those with psychotic disorders, as their problems are understood to be based in their diseased brains, with drugs being required to control the malfunctions.
If professionals really could reliably distinguish those whose problems came from difficult experiences and who could be helped by therapy and self-understanding, from those whose problems were more organic and who could not be helped in a psychological way, then focusing on making such a distinction would be a useful approach. But if their faith in their ability to do this is really a delusion, then what they are really doing is defining everyone on the “psychotic” side of the distinction as being beyond human understanding and help, and so inflicting another blow on those already severely troubled.
It is well known that people dissociate when all of the person’s mind cannot bear facing what happened directly. Later, parts of the person that did not face the experience may be unable to integrate with the parts that did: each feels alien to the other.
It’s what happens next that may be crucial in separating those who will be recognized as having a dissociative disorder from those who will be seen as having a psychotic disorder.
If the person recognizes the “alien” parts of themselves as being just parts of themselves, even if they seem to be disturbing or even “different personalities,” then they have a good chance of seeing themselves, and of having professionals see them, as having PTSD or a dissociative disorder. But if they see the “alien” parts of themselves as being literally aliens, or demons, or CIA agents talking to them through a brain implant, then they will likely be diagnosed as psychotic.
It’s important to notice what’s happening here: it’s the person who feels more strongly alienated from parts of themselves who is likely to make the “psychotic” interpretation about what those parts are — and then it’s that person who will be seen by the mental health system as having a disorder that is understandable only as brain dysfunction.
We might imagine the following exchange:
Person: “I have an alien inside me.”
Mental health professional: “No, what you have inside you is a defective brain, this is brain pathology or illness.”
When we are alienated from someone, we may fail to cooperate with them and actually battle with them, but at least we notice they are a living being. When people are alienated from thoughts, feelings, and parts of themselves, or characters inside themselves, they may fail to work with those parts or integrate them into their identity, but at least they relate to those parts as something alive. What professionals do when they pathologize parts of people or their experiences is to dehumanize them, to see them not as something living that can be related to, but as something that should be exterminated. This is where the alienation becomes compounded.
What’s missing in the professional’s response is an acknowledgment that what the person may have inside them is a very human response to very difficult experiences, and the brain may be simply responding to those experiences. By failing to admit that possibility, recovery becomes more difficult. If the person accepts the professional’s explanation, they may feel no longer inhabited by an alien, but now they are inhabited by pathology, and one that can be expected to be lifelong and requiring lifelong efforts toward ongoing extermination.
Professionals vary of course in when they start seeing evidence of “brain pathology,” versus when they are open to seeing a problem as psychological.
Some will still identify any report of voice hearing as evidence of brain pathology, with no consideration of the possibility that voices could be dissociative.
Some imagine they can use certain criteria to distinguish “dissociative voices” from “psychotic voices” — even though research shows there is no reliable basis for making such a distinction.
Some claim that if a voice is dissociative, then the person will be able to talk to it, while a person cannot talk to a psychotic voice.
The alternative hypothesis is that professionals are simply failing to recognize that alienation exists on a spectrum, and these professionals are mistaking differences in degree of alienation for a categorical distinction that does not exist.
For the purposes of this discussion, let’s say that a person is just dissociative, and not psychotic, if they perceive all the voices they hear (that others don’t) as part of their larger self, while defining someone as “psychotic” if they perceive voices they hear as something other than themselves. (Looked at this way, being “psychotic” is not distinguished from a dissociative problem, but seen as a possible complication that might occur, or a further degree of alienation.)
The tricky issue is that many people who are just dissociative in the sense defined above, actually hear the voices of the other parts of themselves as though they were coming from outside of themselves, from somewhere else in the room for example. They may also “see” parts of themselves as outside of themselves, though they are aware this is just a mental experience and so they are not psychotic. Meanwhile, many people who are “psychotic” in the sense defined above, hear their voices or many of their voices as located inside themselves, though they believe it is not part of themselves — as in the case where they believe that a demon or brain implant has gotten inside of them.
This makes more sense if we think of multiple spectrums: there’s the spectrum of how much a person is alienated from a voice or how much they see it as not themselves, and then there is the spectrum of how much it seems at any given point to be physically inside themselves.
The idea that professionals can define voices as more “psychotic” if people find themselves unable to talk to them also ignores the possibility of a spectrum; it ignores the possibility that inability to talk may be another function of the degree of alienation. We all know, for example, that when people are feeling very alienated from fellow human beings, they often find they are unable to talk with them. Many of us find for example that we can’t talk with people who are too different politically — or even if we are willing to talk, those others will not talk to us!
People in the hearing voices movement, and therapists working with psychosis, commonly find at the outset that people cannot talk to their voices, but with some work, such talk becomes possible, and helpful.
This work is not seen as possible, however, when the person’s initial inability to talk to the voices, and inability to see the voices as part of themselves that can be related to, is interpreted as evidence that the voices are just brain pathology. There is a notion that “one cannot talk to a disease” and so the professional’s interpretation that the voice is brain pathology becomes part of the problem in communication, or compounds it.
I should point out that “dissociation,” like anxiety or depressed mood, is not entirely a bad thing. There are times it is helpful, and some degree of it is part of healthy human functioning. People in the hearing voices network point out that hearing voices — a particular kind of dissociative experience — can also be part of healthy human functioning, though people can also have various kinds of problems with these experiences. Some of those problems reach the level of what is called psychosis — being seriously “out of touch with reality” and/or severely disorganized. But these problems can all potentially be addressed and resolved, by helping people relate to what they are experiencing rather than pathologizing it.
There are now lots of people who have publicly described their journey from being quite truly lost in psychosis, and fully meeting the diagnostic criteria for “schizophrenia,” and who then, as they got more insight, shifted to having experiences that looked something more like a dissociative disorder, and then eventually shifted to not being “disordered” at all. Eleanor Longden is a well-known example. When she was fully “psychotic” she was fully convinced that her voices emanated from physically real beings outside of her who could harm her and her family if she did not obey their commands, and her reasoning process was so bad that at one point she was ready to drill holes into her head to get the voices out, with no insight into the fact she would likely kill herself in the process. Later, she came to recognize the voices as split-off parts of herself, and as she reconciled with those parts, she healed. She tells her story eloquently in her Ted talk and in more detail in this longer version.
I work as a therapist specializing in therapy for psychosis, and while I am not always successful, I have been fortunate enough to help people make similar journeys toward healing.
In the bigger picture, alienation and dissociation is something that happens not just within people, but within and between social groups, tribes, nations, etc. Seeing the “alien other” as just something pathological, something to be exterminated, is not working very well. We need more attention to approaches that recognize the life and the validity in the alien other, and which help people and social groups assert their own needs while also finding ways to recognize and reconcile with the deeper needs of the other. There is reason for hope, so let’s do what we can to nurture the possibilities!
This 6 hour course presents evidence based, practical and humanistic ways to help people recover. For more information or to register, go to this link.
Working with Trauma, Dissociation, and Psychosis: CBT and Other Approaches to Understanding and Recovery - An Online Course
Free Offer: Presentation on “Understanding Psychosis as an Attempt to Solve Problems: Integrating Perspectives on Trauma, Spirituality and Creativity”
Click the link below to access this recording that explores some of the trickiest aspects of "psychosis," and also to receive notices periodically about online courses and webinars that may become available.
http://eepurl.com/cMAgI
Study shows prevalence of dementia among people with schizophrenia is a staggering 28% at age 66 vs 1.3% in 'controls'. Antipsychotics and other medications suggested as possible cause
How Can Soccer Coaching Help People Who Hear Voices?
By Rufus May & Kate Quinn
Through mapping out their voices and supporting voice hearers to talk constructively with their voices, voice hearers can live with their voices in more positive ways.
Nobody Told Me to Do This: What It Means to Be a Dissident Psychiatrist
By Rupinder Legha, MD
The more honestly I have reckoned with my own story—warts and all—the more capable and responsible I have become of understanding the suffering of others.
Mental health professionals are often afraid to address trauma when people are also having experiencing psychosis, but new research proves even more strongly that it is safe and helpful to do so
Websites store cookies to enhance functionality and personalise your experience. You can manage your preferences, but blocking some cookies may impact site performance and services.
Essential cookies enable basic functions and are necessary for the proper function of the website.
Name
Description
Duration
Cookie Preferences
This cookie is used to store the user's cookie consent preferences.